Background
Over the years, the State of Israel has taken a number of initiatives to improve the working conditions of medical residents: their shifts were shortened (from 36 hours to 26); a limit was set of 71.5 working hours per week; a two-hour rest break per shift was stipulated; and the maximum number of shifts per month was limited to six. However, residents report that the specified regulations are not always implemented, that the established regulations are still very demanding, and that their working conditions are difficult. In addition, a third of the residents report working 71.5 hours or more in an average week.
Objectives
The objectives of this study were (1) to review the evidence regarding the maximum work hours of medical residents and their impact on the quality of care and the quality of work life for the trainees; (2) to present up-to-date data on the regulations and work hours in practice of residents in OECD countries; and (3) to identify successful models of relevance to Israel.
Methods
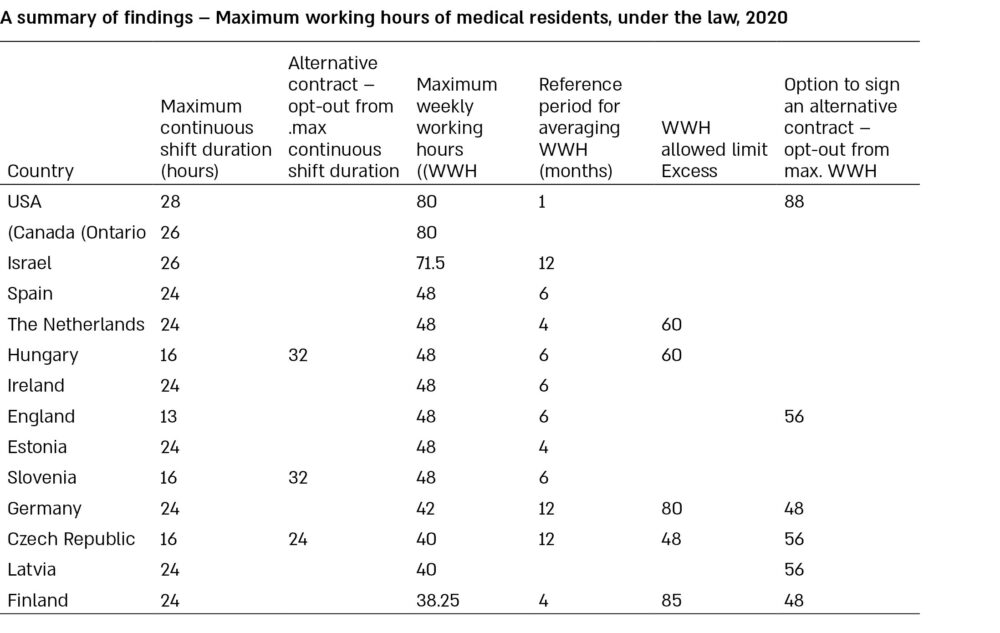
(1) Literature review to identify models of work and their effects on quality of care. (2) Distribution of a questionnaire among experts from 14 different countries for a cross-country comparison of regulations and actual working hours: the United States, Canada, Israel, Spain, the Netherlands, Hungary, Ireland, England, Estonia, Slovenia, Germany, the Czech Republic, Latvia, and Finland.
Findings
Long hours of work and lack of sleep are liable to adversely affect the clinical acumen of medical residents, the quality of patient care they provide, and their own quality of life. The literature review showed five ways that are employed to improve the working conditions and performance of residents: setting a limit on the number of weekly working hours; establishing guaranteed rest breaks; stipulating night float (overnight) shifts in place of consecutive overnight and day shifts; limiting overnight shift frequency; and limiting shift duration.
Empirical studies show that in most cases, when the above-mentioned models were used to ease the burden of long duty hours, improvement was found in one or more of the areas examined (e.g., a reduction in the number of medical errors or an improvement in the quality of life of residents). However, alongside the desired effects, undesirable effects were also reported, such as reduced continuity of patient care and an adverse effect on residency education and training. Of the five ways reviewed in the literature, most of the countries studied decided to tackle the issue by setting a limit on the weekly working hours.
We found two approaches to limiting weekly working hours: (1) The U.S. and Canada set a limit of 80 hours; (2) European countries abide by the EWTD (European Working Time Directive) that sets a limit of 48 weekly working hours (including overnight shifts), averaged over a multi-week period. Some countries find it difficult to comply with this limit, and certain mechanisms have been introduced for exceeding the weekly working hours limit, e.g., using alternative contracts.
Policy recommendations
To improve the work conditions of the residents in Israel and based on the experience of most of the countries studied, we recommend reducing the limit on weekly working hours (the most commonly applied way of improving residents’ work conditions out of the five ways identified in the review). This is the most flexible policy, which allows for the management of working hours in each clinical field taking into account the unique needs of each ward and hospital. The European approach sets a limit of 48 weekly hours; and this may be used as an aspirational goal, while the Ministry of Health (MOH) could periodically set a limit which is appropriate for Israel at that point in time. In light of the international experience, the reduction in maximum work hours should be implemented gradually, in conjunction with the addition of other health professionals (such as physician assistants) who could share the workload with the residents.